
Penoplasty
Professor Hersant - Male Surgery at Paris 16
Penoplasty
The demand for penile augmentation for aesthetic purposes has increased considerably over the last ten years. The probable reason for this increased demand is the explosion of exposure of the genitals in pornographic photos or films on the Internet, in the press and in activities such as hammams and spas (on the increase in Western countries). Phallocentrism is the concept that the penis is central to male identity.
Unlike in ancient Greece, where small phalluses were valued, the male sex is now considered to represent virility, strength and youth. This type of surgery helps to restore a man’s self-confidence, particularly in the flaccid state. This surgery does not improve sexual capacity or erectile function, nor does it improve partner pleasure(1).
Anatomy
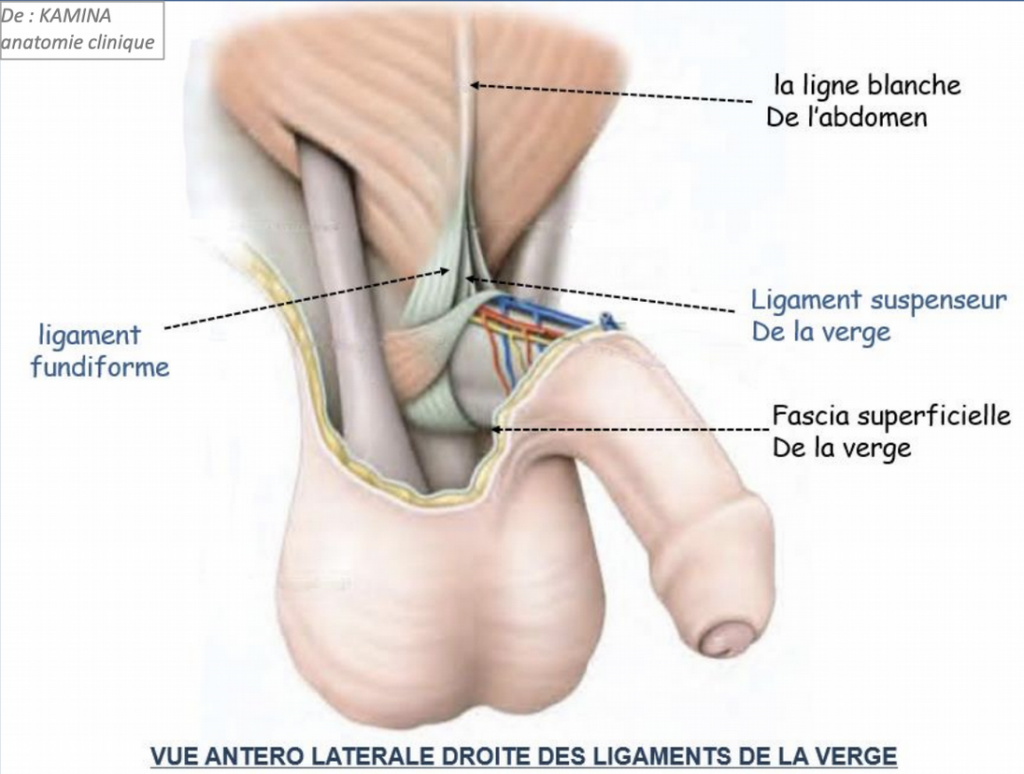
Figure 1: Right anterolateral view of the ligaments of the penis
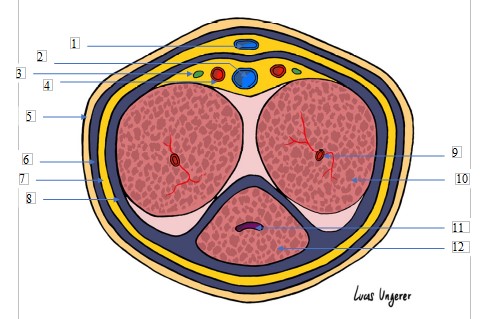
Figure 2: Cross-section of the penis. 1: Superficial dorsal vein; 2: Deep dorsal vein; 3: Dorsal nerve; 4: Dorsal artery; 5: Skin; 6: Superficial fascia (Dartos); 7: Albuginea; 8: Deep fascia (Buck); 9: Deep artery; 10: Cavernous body; 11: Urethra; 12: Corpus spongiosum.
The penis is the male organ of copulation and also the terminal organ of micturition. It is located in front of the pubic symphysis (Figure 1). The urethra runs along its entire length and opens at its distal end into the urethral meatus.
The penis comprises two functionally distinct parts: the root, which is buried in the perineum and fixed, and the body, which is visible and mobile. The root comprises the two pillars and the bulb of the penis. The pillars of the penis correspond to the posterior parts of the corpora cavernosa. Each of the pillars is attached to an ischiopubic branch and to the lower fascia of the urogenital diaphragm. The bulb of the penis corresponds to the posterior part of the corpus spongiosum. It attaches to the underside of the perineal membrane.
The external portion of the penis is located under the pubic symphysis. It has a cylindrical shape with an anterior surface or dorsum of the penis, a posterior surface or urethral surface, and a swollen free end, the glans. The penis has three main erectile components: the two corpora cavernosa, the corpus spongiosum and the glans. The corpora cavernosa abut medially and are separated by a septum. They delimit two longitudinal channels: the upper channel where the deep dorsal vein of the penis runs. The other, lower, is where the corpus spongiosum is inserted. The corpus spongiosum surrounds the urethra and runs in the lower longitudinal groove of the corpora cavernosa. The glans corresponds to the free end of the penis and is covered by the foreskin. It is conical, smooth and pinkish in colour. Its urethral surface has a median groove joining the neck and the external urethral ostium. This is where the frenulum of the foreskin is inserted.
The penis is made up of different envelopes (Figure 2): the thick albuginea which surrounds each of the erectile bodies (the two corpora cavernosa and the corpus spongiosum). The deep fascia of the penis or Buck’s fascia, which surrounds a large cellular space that explains why the sheath can ‘slide’ over the erectile formations. The Dartos or superficial fascia of the penis. And finally, the skin or sheath of the penis.
Be sure to review the anatomy of the ligament with Danino’s new article, as it shows 3 distinct blades.
The penis also has several means of fixation: the body is held in place by its continuity with the root and by the suspensory and fundiform ligaments of the penis. The suspensory ligament is triangular and inserts in front of the pubic symphysis, then spreads and divides into two blades that attach on either side of the corpora cavernosa to the deep fascia of the penis. The fundiform ligament inserts at the lower part of the white line of the abdomen, then crosses the mons pubis. It divides into two blades that pass on either side of the suspensory ligament of the penis.
Indications
The major aesthetic indication is the ‘vestiary complex’, i.e. a cosmetic improvement of the penis at rest of 1 to 4 cm in circumference(2). For patients with a large reserve of sheath skin between the flaccid state and erection, there is the possibility of an increase in length of 1 to 4 cm due to the heaviness of the lipofilling. Surgery is not indicated to improve erection or sexual performance. Although it has been shown that a feeling of confidence about the size of the penis can improve erectile capacity through psychological processes(3).
This surgery can also improve the aesthetics and function of buried pubic hair4. It is mainly performed on patients who have lost weight, causing pubic ptosis, and on neurological patients who are sometimes difficult to probe.
Contraindications
Contraindications to surgical penoplasty must also be identified, in particular any dysmorphophobia or psychiatric disorders. Phimosis and paraphimosis are also contraindications to penoplasty. Other contraindications include Lapeyronie’s disease, erectile dysfunction treated with intra-cavernosal injections, haemostasis disorders and acute local infectious or active inflammatory disease.
Pre-operative preparation
The consultation (at least two before the operation) should identify the patient’s precise expectations.
Four measurements are essential, as are photographs. The length is measured on the dorsal surface of the penis, from the base at the pubo-penile junction to the urinary meat, in the flaccid state, semi-erect or ‘stretched’ (the penis is pulled 3 times) and erect (ask the patient to take the measurement at home when fully erect). The circumference is measured using a flexible tape measure at the middle part of the penis. It is also necessary to look for genital malformations and the existence of plaques that may cause curvature (Lapeyronie’s disease). The foreskin is analysed primarily for circumcision, narrowness or phimosis. Phimosis must always be treated prior to the procedure by posthectomy. If the foreskin is tight or narrow, the procedure should be discussed: partial posthectomy or manual dilatation using silicone dilatation rings.
Dermatological analysis of the glans penis and the balanopreputial fold is necessary for prior treatment or to rule out the procedure: atrophic lichen sclerosus, malignant lesions, condyloma, herpetic disease.
If the patient consults us to improve her sexual capacities, we should explain that female pleasure is essentially clitoral and that the probable ‘G-spot’ is located 4 cm from the vaginal antrum on the anterior surface of the vagina. Female orgasm is in no way dependent on the size of the penis(5). These patients need to be reassured and referred to a urologist and a sexologist. Any erectile dysfunction should be treated by a urologist, as it is also a sign of the onset of cardiovascular disease. Some studies have shown that a 5 cm penis is capable of performing its physiological and reproductive functions(2). The request for lengthening or enlargement must come from the patient and not from his partner.
It is also important to be able to quote average figures for the size of the penis to reassure and situate the patient. The figures given in the press and by pornographers are in fact incorrect. On average, the length of the penis in the flaccid state is 9 cm, and 14 cm when erect; in circumference (this is the perimeter and not the diameter), the size of the penis is 9 cm in the flaccid state and 12 cm when erect(6). These measurements are taken from American and European publications. Contrary to popular rumour, it has been scientifically demonstrated that shoe size is not correlated with penis size. Micropenis occurs when the penis measures less than 8 cm when erect.
Surgical technique
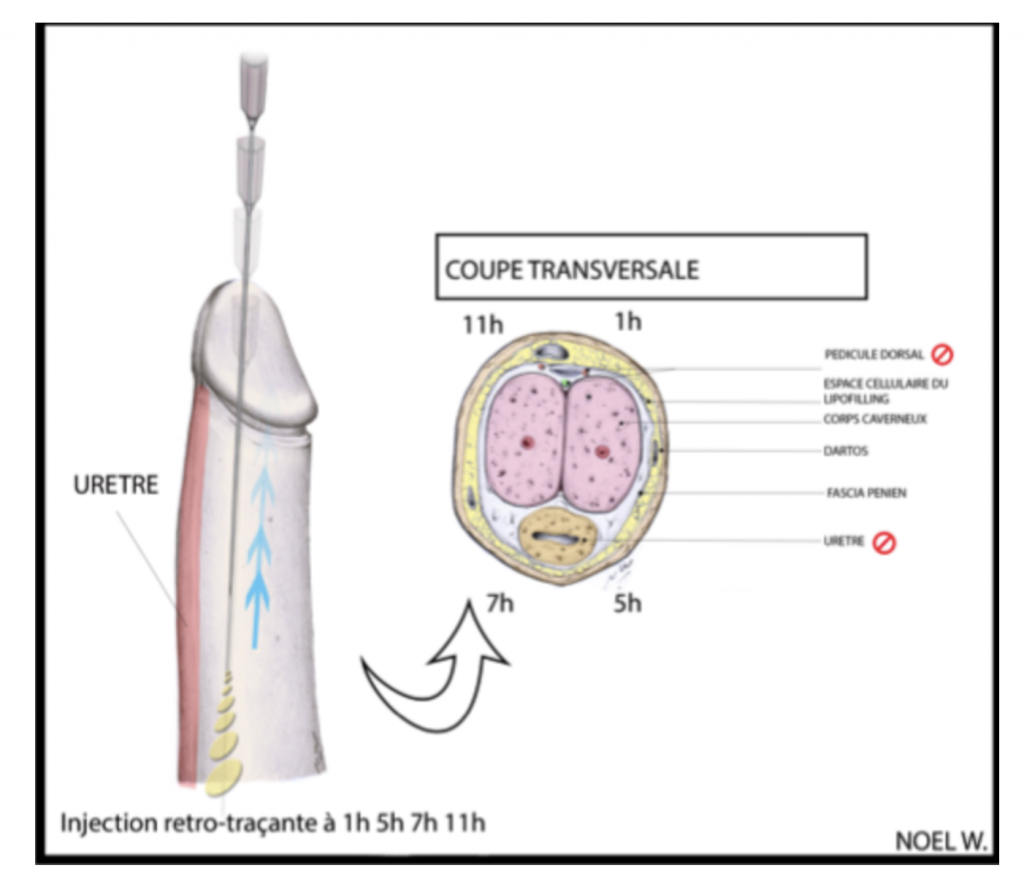
Figure 3: Injection plan and areas at risk during penile lipofilling.
1) Lipofilling of the penis
Lipofilling is performed under general anaesthetic or spinal anaesthetic. An average of 40 to 80 cc of pure fat must be injected to obtain a satisfactory result in the long term. Micro Lipofilling is preferred to avoid cysts and to improve the consolidation of the fat.
Using 2 forceps, the preputial skin is unwrapped and an incision (1mm) is made using an 11 blade or a white needle (pump) in the balloon-preputial fold at 1am, 5am, 7am and 11am, i.e. 4 incisions.
Injection should be avoided at 12 o’clock because of the presence of the dorsal vascular-nervous pedicle of the penis and at 6 o’clock because of the risk of injury to the urethra.
Using a Colman injection cannula, it is necessary to slide through the incisions into the dissection plane, which is avascular (located subcutaneously between the superficial fascia (Dartos) and the deep fascia (Buck’s fascia)) and to be tangential to the penis. The injection is made in a retro-traceable manner (Figure 3). It is also possible to inject between Buck’s fascia and the albuginea, provided that the injection is only lateral. One trick for checking whether you are injecting in this plane is to avoid palpating the cannula during the pinch test. This plane of injection avoids migration of the product. Suturing the incisions should be avoided.
Massage is recommended in order to distribute the fat correctly, and do not hesitate to ‘knead’ between the 2 hands in the transverse plane in order to avoid the appearance of fatty deposits, which may require a repeat operation. A modelling dressing is necessary. Urinary catheterisation is not recommended.
2) Plasty to lengthen the penis
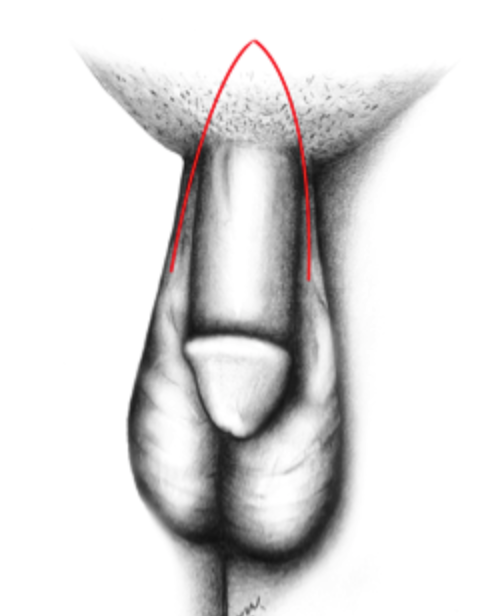
Figure 4 : V-Y lengthening of the penis
Section of the suspensory ligament and V-Y plasty (Figure 4).
The suspensory and fundiform ligament of the penis is extended between the lower part of the pubic symphysis (4 to 5 cm below the skin) and the dorsal surface of the penis.
A V-shaped incision must be made halfway between the lower part of the symphysis and the penis to avoid damaging the vascular and neural pedicle of the penis and to lower the V towards the scrotum. Care must be taken laterally to the spermatic cords. The ligament is resected transversely, subtotally, to maintain erectile stability (Figure 3). This section allows a lengthening of 1 to 2 cm. The space left by the dissection may cause haematoma or secondary fibrosis, and must be filled by suturing in several planes or by applying biological glue. There is an advantage in interposing a small flap of fat from the pubis in this space to prevent adhesions from forming, which could ultimately lead to shortening of the penis. Some patients use paediatric testicular prostheses to act as a ‘spacer’ in this dead space(7).
Closure is achieved by means of a V-Y plasty in order to increase the length of the cutaneous part.
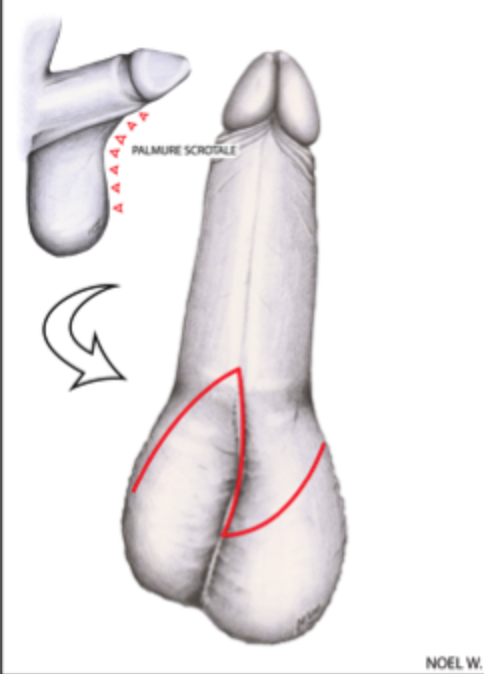
Figure 5: Incision areas for scrotal Z-plasty
3) Scrotal Z-plasty (Figure 5)
At the penile-scrotal junction, there is a skin adhesion or scrotal web which can be the subject of a large Z-plasty in order to increase the length of the skin. The central bar of the Z should be placed on the midline of this web. The dissection must be carried out in the avascular plane between the dartos and the vagina. A simple suture using separate stitches will suffice.
4) Decubitus of the penis
The above techniques should be combined with a cure for pubic ptosis if necessary. The cure of pubic ptosis consists of a cutaneous fatty resection without detachment by placing the scar above the pubic bone. This surgery is necessary for patients with massive weight loss or for ‘neurological’ patients who are difficult to probe.
Post-operative care
Lipofilling of the penis
Sexual activity is contraindicated for 3 weeks, including masturbation. Intimate hygiene is essential and washing with soap and water in the shower is a must. Level 1 and 2 painkillers must be prescribed. NSAIDs should be avoided. Antibiotic therapy is not recommended(32). Scar care with water, soap and physiological saline should be carried out by a nurse at home.
Plasty to lengthen the penis
Sexual activity is contraindicated for 3 weeks, including masturbation. Intimate hygiene is essential and washing with soap and water in the shower is a must. Level 1 and 2 painkillers must be prescribed. NSAIDs should be avoided. Antibiotic therapy is not recommended(23). Scar care with water, soap and saline should be carried out by a nurse at home.
Scrotal Z-plasty
Sexual activity is contraindicated for 3 weeks, including masturbation. Intimate hygiene is essential and washing with soap and water in the shower is a must. Level 1 and 2 painkillers must be prescribed. NSAIDs should be avoided. Antibiotic therapy is not recommended(23). Scar care with soap, water and saline should be carried out by a home care nurse.
Results
Lipofilling of the penis
The circumference can increase by 1 to 4 cm and by ‘weighing down’ the penis, lipofilling can allow an increase of 1cm to 4 cm in length 2-3. Patients should be warned that on average 50% of the fat is likely to disappear and that post-operative oedema disappears within 6 weeks. Enlargement may therefore appear impressive in the immediate post-operative period, but this is not the final result.
Lengthening of the penis and scrotal Z-plasty
By combining all these techniques, section of the suspensory ligament combined with a V-Y plasty, a Z-plasty on the penoscrotal skin and lipofilling, we can hope to achieve an elongation of 2 to 3 cm. It is preferable to give the patient a target of 1 or 2 cm to prevent possible dissatisfaction, which remains the main complication of this surgery.
Complications
Few complications have been reported in the literature234. The main complication is poor fat distribution during penile enlargement, with the patient experiencing fatty deposits. A moderate injection (40ml) with a modelling massage to be repeated by the patient according to the pain, as well as strict sexual abstinence, help to avoid these fatty deposits.
In the event of repeated erections, a treatment may be used, but the risk of this type of treatment is not without consequences (beta-blocker, Androcur).
Seroma is rare, but may appear a few weeks after the operation at the root of the penis. Infection is rare, but possible. It may require surgical drainage. Changes in sensitivity may also occur, but these are usually transient. Finally, insufficient results are a possible complication.
In the case of V-Y plasty, disunions, haematomas and skin necrosis may occur if the flaps are not optimally designed. Caution: the main risk factors are smoking and diabetes, which are contraindications to this type of operation. There may also be a reduction in the size of the penis due to the significant retraction caused by fibrosis following section of the suspensory ligament. It is essential to fill in the dead space.
With Z-plasty, haematoma and disunion are the main complications. The main risk factors are smoking and diabetes, which are contraindications.
Bibliography
1. Abecassis M, Berreby S, Boccara D. [Penile enhancement surgery: widening and lengthening lipopenisculpture]. Ann Chir Plast Esthet. 2010;55(2):135-142. doi:10.1016/j.anplas.2009.02.001
2. Dillon BE, Chama NB, Honig SC. Penile size and penile enlargement surgery: a review. Int J Impot Res. 2008;20(6):519-529. doi:10.1038/ijir.2008.14
3. Panfilov DE. Augmentative phalloplasty. Aesthetic Plast Surg. 2006;30(2):183-197. doi:10.1007/s00266-004-0153-y
4. Alter GJ. Pubic contouring after massive weight loss in men and women: correction of hidden penis, mons ptosis, and labia majora enlargement. Plast Reconstr Surg. 2012;130(4):936-947. doi:10.1097/PRS.0b013e318262f57d
5. Costa RM, Miller GF, Brody S. Penis size and vaginal orgasm. J Sex Med. 2013;10(11):2875-2876. doi:10.1111/jsm.12281
6. Veale D, Miles S, Bramley S, Muir G, Hodsoll J. Am I normal? A systematic review and construction of nomograms for flaccid and erect penis length and circumference in up to 15,521 men. BJU Int. 2015;115(6):978-986. doi:10.1111/bju.13010
7. Shaeer O. Supersizing the penis following penile prosthesis implantation. J Sex Med. 2010;7(7):2608-2616. doi:10.1111/j.1743-6109.2010.01723.x